
In the mid-2000s, getting medical image data from one provider to another was difficult (to say the least). We invented a technology which we call fileshare which made it easy to send and receive medical imaging data between providers. No email attachments were needed, no viruses could be transmitted. All the sender and receiver had to have was a computer, an Internet connection, and a standard browser such as Microsoft’s IE. With that they could exchange data in a safe, secure, authenticated and HIPAA compliant manner. Fileshare continues to be used in medical applications at places such as the Indiana University School of Medicine, Louisiana State University, and others.

Long before the advent of open EMR interface engines we worked with a client who needed access to clinical patient demographic data for their application. They needed an interface to any EMR/EHR system that their clients used and they needed an interface that was straightforward, simple, reliable. Oh, and it also had to have an internal mapping engine that automatically transformed data from a given EMR/EHR into a form useful to their application.
We built it for them.
We built it for them.
Supporwell understands business processes as well as it understands technical processes. And it understands which is which. When a client wanted us to educate computer science graduate students on the business opportunities of cloud computing, we were glad to comply. The question of whether to insource or outsource is a perpetual one in business along with its parallel questions of whether to lease, buy, or rent capital equipment. Cloud computing is a business tool made possible by developments in computing, infrastructure, and standards.
Why not educate tomorrow’s programmers on today’s business needs before they even graduate?
Why not educate tomorrow’s programmers on today’s business needs before they even graduate?
When a small Silicon Valley-based healthcare startup partnered with a much larger software development company, someone had to manage the corporate cultural impedance. It didn’t help that the two companies were half a world apart geographically, either. We stepped in and gathered the startup’s specifications and needs and turned to the software development house to turn those specifications into a working system. We managed that by reaching out to the startup’s customers with onsite visits, bringing what we learned there back to the startup, turning what we needed into a development roadmap, and managing the whole process to a successful outcome.
And, yes, that image to the left is an actual shot of an actual whiteboard used on the project. Keeping it real is what we do at Supporwell.
And, yes, that image to the left is an actual shot of an actual whiteboard used on the project. Keeping it real is what we do at Supporwell.
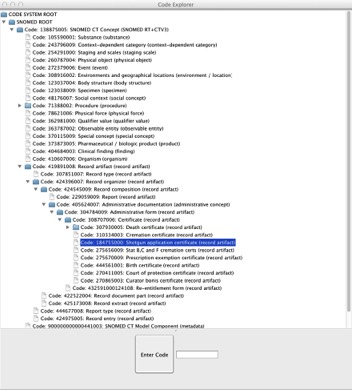
ICD-9, ICD-10, SNOMED, RXNORM, oh-my! We don’t just develop software for our clients, we develop it for our own in-house use as well. We use it to rapidly produce proof-of-concept systems, for research, and to find out if there is just another, better, way.
For example, our Code Explorer enables interactive exploration of the various coding systems used in our industry, imposing hierarchy where necessary and pruning specifics up the tree to more general concepts.
You can’t build solutions until you understand your industry.
For example, our Code Explorer enables interactive exploration of the various coding systems used in our industry, imposing hierarchy where necessary and pruning specifics up the tree to more general concepts.
You can’t build solutions until you understand your industry.

Meaningful Use certification is a huge incentive for information technology system adaptation in the clinical and hospital environment. Here is what one client had to say about our help in getting their system certified:
The entire team headed [by] Greg Travis here in Palo Alto has pulled off a great feat by completing the MU certification changes and tests in record time. I can't praise them enough! It was far from a cake-walk: there were times when they were working late and on weekends and were frustrated with me but they have been extremely professional and have pulled it off.
Sanjeev Dharap

How do you assure uptake of mobile applications by providers and their staff? You have to make sure they find value in the technology. The clinical environment is relentlessly pragmatic and has no time for anything that gets in the way of delivering care to patients.
When we were designing a tablet-based patient and practice management system we knew it had no chance if either patients or clinical staff saw no value. It had to be intuitive, it had to be easy, and it had to replace the ways in which they had been doing things. Which meant it had to be better than what they had already.
We knew we had one chance at acceptance. So we visited clinics all over the country and watched them at work. We saw how they did their jobs, how they used technology, and what their challenges were. We also saw what was working well.
By the time we rolled the application out to the nursing staff and the patients, it already fit into their well-established workflow in a familiar and non-intrusive way. It’s not just about technology for technology’s sake.
It has to make things better.
When we were designing a tablet-based patient and practice management system we knew it had no chance if either patients or clinical staff saw no value. It had to be intuitive, it had to be easy, and it had to replace the ways in which they had been doing things. Which meant it had to be better than what they had already.
We knew we had one chance at acceptance. So we visited clinics all over the country and watched them at work. We saw how they did their jobs, how they used technology, and what their challenges were. We also saw what was working well.
By the time we rolled the application out to the nursing staff and the patients, it already fit into their well-established workflow in a familiar and non-intrusive way. It’s not just about technology for technology’s sake.
It has to make things better.

It’s not all healthcare IT (although that is our passion). Supporwell has a long history in advanced research and development for the computer networking community with a focus on Cybersecurity. Here Supporwell Managing Partner Gregory Travis, then a fellow at the Indiana University Center for Applied Cybersecurity Research (CACR), gave a talk about the Department of Defense’s rush to adopt IPv6 and the potential harms that might accrue deploying an immature technology on the battlefield. The title of Mr. Travis’ presentation here is If We Fail, People Die: Sense, Security, and Nonsense about IPv6